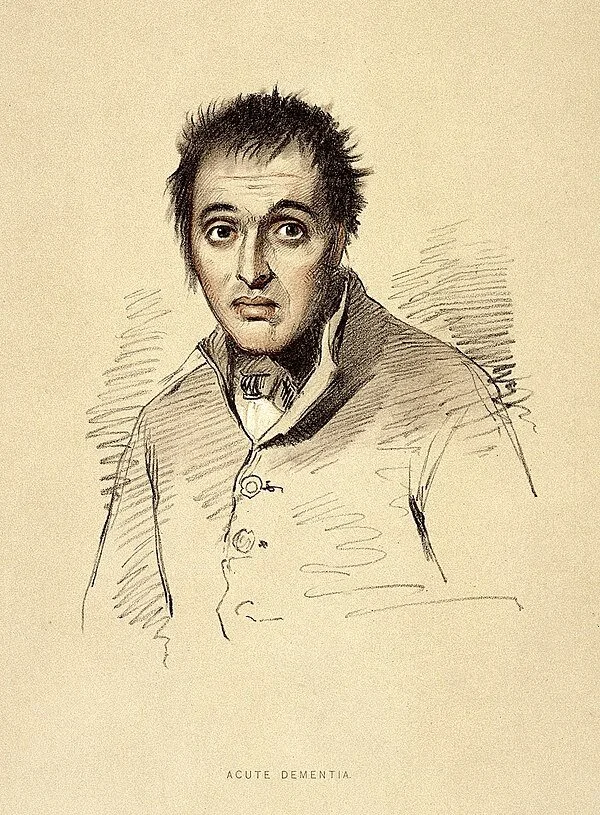
Self-portrait of American figurative artist William Utermohlen, created after he was diagnosed with Alzheimer's disease, in 1995. He experienced memory loss beginning in 1991. After his diagnosis he began creating self-portraits and continued it for another six years, until he made the final self-portraits in 2001. He died in 2007. In the years after the publication of his works in The Lancet in 2001, Utermohlen's self-portraits have been displayed in several exhibitions. His self-portraits inspired the 2019 short film Mémorable.
If you listen to the nation’s largest Alzheimer’s disease advocacy organizations, you might think everyone living with Alzheimer’s wants unfettered access to Aduhelm, a controversial new treatment produced by the Cambridge, Mass., biotech company Biogen.
But you’d be wrong.
Opinions about Aduhelm (also known as aducanumab) in the dementia community are diverse, ranging from “we want the government to cover this drug” to “we’re concerned about this medication and think it should be studied further.”
The Alzheimer’s Association and UsAgainstAlzheimer’s, the most influential advocacy organizations in the field, are in the former camp.
Both are pushing for Medicare to cover Aduhelm’s $28,000 annual per-patient cost and fiercely oppose the Centers for Medicare & Medicaid Services’ January proposal to restrict coverage only to people enrolled in clinical trials. Nearly 10,000 comments were received on that proposal, and a final decision is expected in April.
“With respect, we have no more time for debate or delay,” the Alzheimer’s Association national Early-Stage Advisory Group wrote in a Feb. 10 comment. “Every passing day without access to potential treatments subjects us to a future of irreversible decline.” For its part, UsAgainstAlzheimer’s called CMS’ proposal “anti-patient.”
Yet the scientific evidence behind Aduhelm is inconclusive, its efficacy in preventing the progression of Alzheimer’s remains unproved, and there are concerns about its safety. The FDA granted accelerated approval to the medication last June but ordered the drugmaker, Biogen, to conduct a new clinical trial to verify its benefit. And the agency’s decision came despite a 10-0 recommendation against doing so from its scientific advisory committee. (One committee member abstained, citing uncertainty.)
Other organizations representing people living with dementia are more cautious, calling for more research about Aduhelm’s effectiveness and potential side effects. More than 40 percent of people who take the medication have swelling or bleeding in the brain — complications that need to be carefully monitored.
The Dementia Action Alliance, which supports people living with dementia, is among them. In a statement forwarded to me by CEO Karen Love, the organization said, “DAA strongly supports CMS’s decision to limit access to aducanumab to people enrolled in qualifying clinical trials in order to better study aducanumab’s efficacy and adverse effects.”
Meanwhile, Dementia Alliance International — the world’s largest organization run by and for people with dementia, with more than 5,000 members — has not taken a position on Aduhelm. “We felt that coming out with a statement on one side or another would split our organization,” said Diana Blackwelder, its treasurer, who lives in Washington, D.C.
Blackwelder, 60, who was diagnosed with early-onset Alzheimer’s in 2017, told me, “To say that millions of people afflicted with a disease are all up in arms against CMS’s proposal is just wrong. We’re all individuals, not a collective.”
“I understand the need for hope,” she said, expressing a personal opinion, “but people living with dementia need to be protected as well. This drug has very serious, frequent side effects. My concern is that whatever CMS decides, they at least put in some guardrails so that people taking this drug get proper workups and monitoring.”
The debate over Medicare’s decision on Aduhelm is crucial, since most people with Alzheimer’s are older or seriously disabled and covered by the government health program.
To learn more, I talked to several people living with dementia. Here’s some of what they told me:
Jay Reinstein, 60, is married and lives in Raleigh, N.C. He was diagnosed with early-onset Alzheimer’s disease three years ago and formerly served on the national board of directors of the Alzheimer’s Association.
“I understand [Aduhelm] is controversial, but to me it’s a risk I’m willing to take because there’s nothing else out there,” Reinstein said, noting that people he’s met through support groups have progressed in their disease very quickly. “Even if it’s a 10 percent chance of slowing [Alzheimer’s] down by six months, I am still willing to take it. While I am progressing slowly, I want more time.”
Laurie Scherrer of Albertville, Ala., was diagnosed with early-onset Alzheimer’s and frontotemporal dementia in 2013, at age 55.
Early on, she was prescribed Aricept (donepezil), one of a handful of medications that address Alzheimer’s symptoms. “I became totally confused and disoriented, I couldn’t think, I couldn’t concentrate,” she told me. After stopping the medication, those symptoms went away.
“I am not for CMS approving this drug, and I wouldn’t take it,” Scherrer said. At discussion groups on Aduhelm hosted by the Dementia Action Alliance (Scherrer is on the board), only two of 50 participants wanted the drug to be made widely available. The reason, she said: “They don’t think there are enough benefits to counteract the possible harms.”
Rebecca Chopp, 69, of Broomfield, Colo., was diagnosed with early-onset Alzheimer’s in March 2019. She’s a former chancellor of the University of Denver.
Chopp is a member of a newly formed group of five people with dementia who meet regularly, “support one another,” and want to “tell the story of Alzheimer’s from our perspective,” she said.
Two people in the group have taken Aduhelm, and both report that it has improved their well-being. “I believe in science, and I am very respectful of the large number of scientists who feel that [Aduhelm] should not have been approved,” she told me. “But I’m equally compassionate toward those who are desperate and who feel this [drug] might help them.”
Chopp opposes CMS’s decision because “Aduhelm has been FDA-approved and I think it should be funded for those who choose to take it.”
Joanna Fix, 53, of Colorado Springs was diagnosed with early-onset Alzheimer’s disease in October 2016. She, too, developed serious complications after taking Aricept and another dementia medication, Namenda (memantine).
“I would love it if tomorrow somebody said, ‘Here’s something that can cure you,’ but I don’t think we’re at that point with Aduhelm,” Fix told me. “We haven’t been looking at this [drug] long enough. It feels like this is just throwing something at the disease because there’s nothing else to do.”
“Please, please take it from someone living with this disease: There is more to life than taking a magic pill,” Fix continued. “All I care about is my quality of life. My marriage. Educating and helping other people living with dementia. And what I can still do day to day.”
Phil Gutis, 60, of Solebury, Penn., has participated in clinical trials and taken Aduhelm for 5½ years after being diagnosed with early-onset Alzheimer’s in 2016.
He’s convinced the medication has helped him. “I don’t know how to describe it other than to say my head feels so much clearer now,” he told me. “I feel much more capable of doing things now. It’s not like I’ve gained my memories back, but I certainly haven’t deteriorated.”
Gutis thinks CMS’s proposed restrictions on Aduhelm are misguided. “When the FDA approved it, there was this sense of excitement — oh, we’re getting somewhere. With the CMS decision, I feel we are setting the field back again. It’s this constant feeling that progress is being made and then — whack.”
Christine Thelker, 62, is a widow who lives alone in Vernon, British Columbia. She was diagnosed with vascular dementia seven years ago and is a board member for Dementia Advocacy Canada, which supports restrictions on Aduhelm’s availability.
“Most of us who live with dementia understand a cure is not likely: There are too many different types of dementia, and it’s just too complicated,” Thelker told me. “To think we’re just going to take a pill and be better is not realistic. Don’t give us false hope.”
What people with Alzheimer’s and other types of dementia need, instead, is “various types of rehabilitation and assistance that can improve our quality of life and help us maintain a sense of hope and purpose,” Thelker said.
Jim Taylor of New York City and Sherman, Conn., is a caregiver for his wife, Geri Taylor, 78, who has moderate Alzheimer’s. She joined a clinical trial for Aduhelm in 2015 and has been on the drug since, with the exception of about 12 months when Biogen temporarily stopped the clinical trial. “In that period, her short-term memory and communications skills noticeably declined,” Jim Taylor said.
“We’re convinced the medication is a good thing, though we know it’s not helpful for everybody,” Taylor continued. “It really boosts [Geri’s] spirits to think she’s part of research and doing everything she can.
“If it’s helpful for some and it can be monitored so that any side effects are caught in a timely way, then I think [Aduhelm] should be available. That decision should be left up to the person with the disease and their care partner.”
Judith Graham is a Kaiser Health News reporter.

Biogen headquarters in Cambridge, one of the world’s biotech centers.